Adult and Child ENT Care
Ear Tubes
 Ear infections are common in children and by the age of five, most children have experienced at least one episode. Majority of ear infections resolve either on their own or with antibiotic treatment. But sometimes ear infections and fluid in the middle ear may become a chronic problem leading to hearing loss, behavior and speech problems, or other issues. Placement of ear tubes is considered in these situations.
Ear infections are common in children and by the age of five, most children have experienced at least one episode. Majority of ear infections resolve either on their own or with antibiotic treatment. But sometimes ear infections and fluid in the middle ear may become a chronic problem leading to hearing loss, behavior and speech problems, or other issues. Placement of ear tubes is considered in these situations.
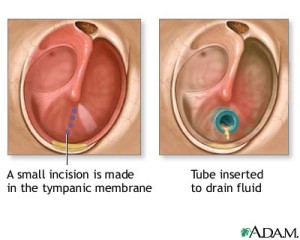
Ear tubes are tiny cylinders placed through the ear drum to allow air into the middle ear. Short- term tubes are smaller and typically stay in place for six months to 2 year before falling out on their own. Long-term tubes are larger and have flanges (T-tubes) that secure them in place for a longer period of time. Long-term tubes may fall out on their own or require removal.
Ear tubes are more common in children for recurrent acute ear infections and/or persistent middle ear fluid with hearing loss. These conditions can occur in teens and adults as well. Other indications for ear tube placement include dysfunction of the eustachian tubes and barotrauma (often seen with changes in altitude with flying or scuba diving.)
Ear tube placement is the most common pediatric procedure performed with anesthesia. In appropriately selected patients, ear tubes can: Reduce risk of future ear infection; resolve hearing loss due to middle ear fluid, improve speech difficulty, and improve behavior and sleep issues.
Myringotomy with insertion of ear tubes is an extremely common and safe procedure with minimal complications. Possible complications include perforation, scarring, infection, and retained or early extrusion of the tube.
- Perforation: A hole in the ear drum may persist after an ear tube comes out. The chance of a persistent hole is higher when a long term tube (T-tube) is used or multiple ear tubes have been placed. The hole can be repaired through a surgical procedure called a tympanoplasty or myringoplasty depending on the size of the hole.
- Scarring: Irritation of the ear drum including recurrent ear infections or repeated insertion of ear tubes can cause scarring of the ear drum. In majority of cases, this causes no problem with hearing.
- Infection: Ear infections can still occur after insertion of ear tubes. These infections are typically less frequent and are easier to treat with ear drops.
- Retained or early extrusion of the tube: Tubes may extrude early with re-accumulation of fluid and need for repeat surgery. Ear tubes may remain too long and result in perforation or require removal.
If you or your child has experienced repeated or severe ear infections, an infection that has not resolved with antibiotics, hearing loss due to fluid in the middle ear, barotrauma, or have eustachian tube dysfunction; our doctors at C/V ENT Surgical Group, serving the greater Los Angeles and San Fernando Valley area, will perform a thorough evaluation and discuss if you or your child is a candidate for ear tubes.
Tonsils and Adenoids
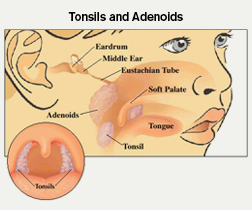
Tonsils and Adenoids Tonsils and adenoids are part of the immune system. At times, they can become more of a liability than an asset by causing airway obstruction or repeated infections. The tonsils are two masses of tissue that are located in the back of the throat, behind and above the tongue. The tonsils can be visualized in the back of the mouth. The adenoids are located behind the nose and upper throat in between the eustachian tubes. The adenoids are not visible through the mouth or nose without special instruments.
 Tonsillitis is an infection of the tonsils with symptoms including: Red and swollen tonsils, a white or yellow coating on the tonsils, voice change due to swelling, sore throat, possible ear pain, painful swallowing, enlarged lymph nodes in the neck, fever, and bad breath. Severe or chronic infections can result in abscesses around the tonsils (peritonsillar and parapharyngeal abscess) and chronic tonsillitis. Bacterial infections of the tonsils are initially treated with antibiotics.
Tonsillitis is an infection of the tonsils with symptoms including: Red and swollen tonsils, a white or yellow coating on the tonsils, voice change due to swelling, sore throat, possible ear pain, painful swallowing, enlarged lymph nodes in the neck, fever, and bad breath. Severe or chronic infections can result in abscesses around the tonsils (peritonsillar and parapharyngeal abscess) and chronic tonsillitis. Bacterial infections of the tonsils are initially treated with antibiotics.
Tonsils and adenoids maybe enlarged without symptoms of tonsillitis. Enlargement of the adenoids may cause difficulty with breathing through the nose, runny nose, and frequent sinus infections. Enlargement of the tonsils and adenoids can cause sleep apnea with loud snoring and gasping for air. Other symptoms include mouth breathing, noisy breathing during the day, and recurrent ear infections. Such obstruction to breathing causes snoring and poor quality sleep that leads to daytime sleepiness, and may even cause behavioral and school issues in some children.
Surgery is reserved for cases of recurrent infections despite antibiotic therapy and/or difficulty with breathing due to the size of tonsils and/or adenoids. Removal of the adenoids maybe indicated in cases of recurrent ear infections or sinusitis in children. In adults, the possibility of cancer or a tumor may be another reason for removing the tonsils and adenoids.
Our specialists at C/V ENT Surgical Group have expertise in treating both pediatric and adult conditions affecting the tonsils and adenoids. They will perform a thorough evaluation and explain both surgical and non-surgical options available based on your specific case.
Tongue-tie (Ankyloglossia)
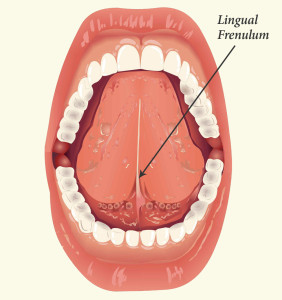 Tongue-tie or ankyloglossia is a problem with a thin strip of tissue under the tongue. This tissue is called the frenulum. It connects from the underside of the tongue to the floor of the mouth. You can see it if you look under your tongue in a mirror. Some children are born with a frenulum that is too short and tight, which and may cause tongue mobility problems. This can cause problems with speech and eating.
Tongue-tie or ankyloglossia is a problem with a thin strip of tissue under the tongue. This tissue is called the frenulum. It connects from the underside of the tongue to the floor of the mouth. You can see it if you look under your tongue in a mirror. Some children are born with a frenulum that is too short and tight, which and may cause tongue mobility problems. This can cause problems with speech and eating.
Indications for treatment depend on age. Infants with tight-tie can have trouble sucking and latching on with resultant poor weight gain. Nursing mothers who experience significant pain while nursing or whose baby has trouble latching on should have their child evaluated for tongue tie. Tongue tie can be an underlying cause of feeding problems and can also lead to abandonment of breast feeding. Toddlers and older children with tongue-tie may have difficulty with articulation of sounds such as “t,” “d,” “z,” “s,” “th,” “n,” and “l.” Children with tongue tie commonly have a V-shaped notch at the tip of the tongue, difficulty with sticking out their tongue, difficulty with touching the roof of the mouth, and difficulty moving the tongue from side to side.
Tongue-tie surgery is a simple procedure. For infants, the procedure may be done in the office. Older children will often require general anesthesia. While frenulectomy is relatively simple, it can yield big results. Our otolaryngologists at C/V ENT Surgical Associates will guide you through the evaluation and determine if your child will benefit from a frenulectomy.